Can Azacitidine be administered at home? The Spanish experience
Written by Manuela Rotstein
A new project was trialled for more than two years by nurses from home-care units in Spain: 'Azacitidine (Vidaza) administration at home'.
Now it has been rolled out to include most of the hospitals in Spain administering Azacitidine. It was initially undertaken by nurses, not necessarily haematology nurses, who would visit patients at home usually by taxi from the hospital.
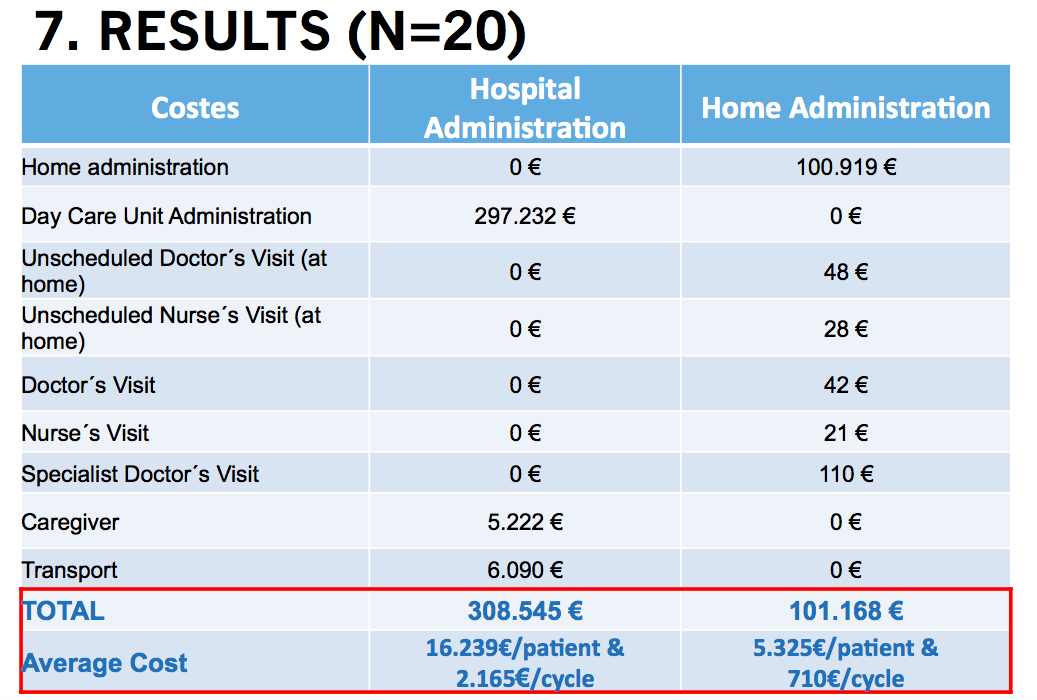
The economic savings were shown to be vast, saving around one-third compared to hospital administration. This equated to around 100.000 euros per year per patient.
See comparison below and download the full presentation here
Receiving Azacitidine at home increased patients' satisfaction
The patient videos and reports demonstrated clearly the increased level of patient satisfaction and improved quality of life for this patient group. Discussions around this included other units adopting the practice of caregivers trained to give Azacitidine at home once they had collected from the hospital on daily basis. This again showed a significant positive impact on patients who, for example, were already fatigued.